

Carpal tunnel syndrome is the most common peripheral nerve entrapment syndrome. It is due to the pressure of the median nerve in the inflexible carpal tunnel creating a series of symptoms in the fingers to the wrist to the forearm while often the symptoms involve the entire upper limb.
Anatomy
Clinical picture
Paresthesias, hypoesthesia, numbness in the distribution of the median nerve, i.e. in the 3.5 fingers (thumb, index, middle and the rostral side of the paramembrane), unspecified wrist and finger pains quite often with extension to the forearm.
Clinical examination
The classic clinical findings include a positive Tinel test (impact of the carpal tunnel with accompanying manifestation of more intense symptoms of paresthesia and hemodia), the Falen Test (pressure of the carpal tunnel with prolonged overflexion of the wrist for 30-60 sec is considered positive at the onset of hemodia symptoms .
Rationale
• Diabetes
• Alcoholism
• Fibular fracture
• Rheumatoid arthritis
• Hypothyroidism
• Pregnancy/Horse (often transient syndrome)
• Occupational disease (manipulators, excessive computer use)
• Genetic predisposition
Epidemiology
Carpal tunnel syndrome is more common in women about 9:1 compared to men, the average age of patients who will undergo median nerve decompression surgery with carpal tunnel syndrome is 54 years.
Diagnostic examinations
The electrophysiological test is the most common and valid diagnostic tool for the diagnosis of carpal tunnel syndrome. The electromyogram should be performed and taken into consideration with the clinical signs for a safe preoperative test.

Differential diagnosis
• Cervical radiculitis A6 (CMD A5-A6) diagnosis with MRI AMSS
• Ganglion cyst palmar in the wrist area
Treatment
• Conservative : Night splints to avoid wrist flexion and extension, rest and avoidance of intense manual activity, administration of steroids and NSAID treatment. In more intense symptoms, corticosteroid injection into the carpal tunnel is used.

Surgical treatment : It should be decided in case of non-response to conservative treatment, when we have worsening nervous symptoms with accompanying night pain with paresthesias, hemodia and above all with a positive result of a neurophysiological test with an electromyogram.
The surgery is performed under local anesthesia and lasts from 15-30 minutes.
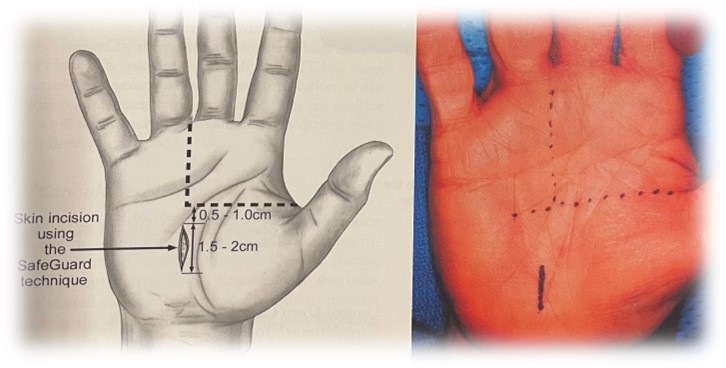
A 1.5-2 cm skin incision with the MIS (Minimal Invasive Surgery) technique is followed by identification and opening of the transverse ligament, careful release of the median nerve, taking into account anatomical variations to avoid iatrogenic damage – complications.

Dr. Angelidakis Ioannis, PhD, University of Crete
Orthopedic Surgeon, Apt. Responsible Orthopedic Department, Creta InterClinic, HHG Group Member

Creta InterClinic Private Clinic
Member of the HHG Group
63 Minoos, 713 04
HERACLION, Crete
Tel. 2810 373800
Fax: 2810 314900
www.cic.gr, e-mail: [email protected]
Source :Skai
I have worked in the news industry for over 10 years. I have a vast amount of experience in covering health news. I am also an author at News Bulletin 247. I am highly experienced and knowledgeable in this field. I am a hard worker and always deliver quality work. I am a reliable source of information and always provide accurate information.








